Foundation | Movement & Injury Science
If you’ve had lateral knee pain as a runner or cyclist, someone has almost certainly told you that your IT band is tight and that you need to foam roll it. You’ve probably done this and grimaced through the pain, dutifully crushing the outside of your thigh against a piece of dense foam before and after runs. Maybe it helps for a few hours. Maybe it doesn’t. Either way, the pain keeps coming back.
There’s a reason for that. The standard explanation of IT band syndrome, the treatment approach that follows from it, and the basic biomechanical model most athletes and even many clinicians are working from are all wrong. Not slightly off. Structurally wrong.
I realize that’s a strong claim. Let me walk through it.
Friction is the old story
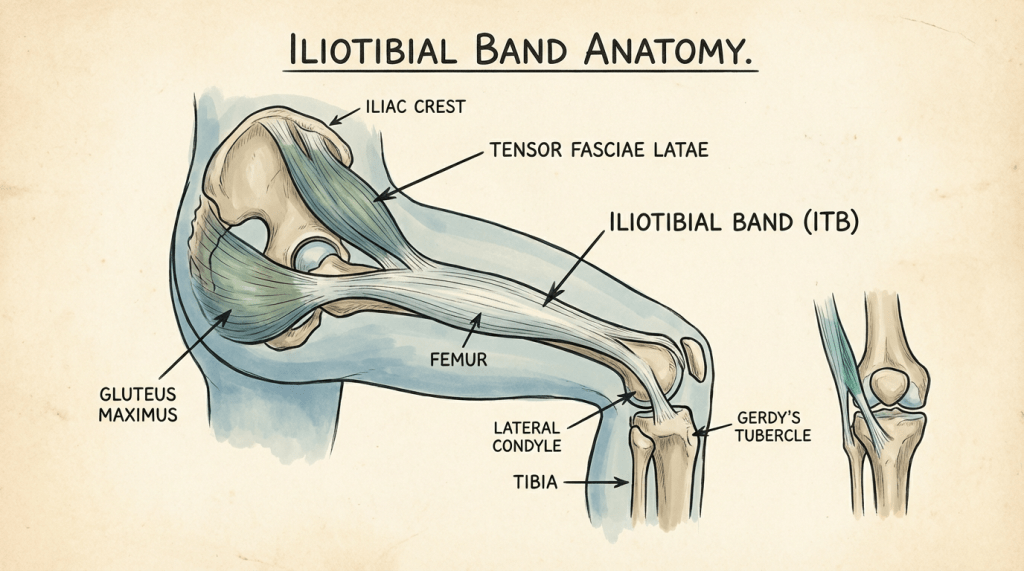
The traditional model, and the one you’ll still find in most running injury articles and a surprising number of textbooks, goes like this: the iliotibial band is a thick strap of tissue that runs along the outside of your thigh from the hip to just below the knee. When you’re running running, it slides back and forth over the lateral femoral epicondyle (the bony bump on the outside of your femur). This repetitive sliding creates friction, which causes inflammation, which causes pain. Hence the old name: “IT band friction syndrome.”
This model makes the solution seem incredibly obvious. The band is tight and rubbing, so you stretch it, foam roll it, and maybe get some manual therapy to loosen it up. Everything is devoted to stretching out that band. Reduce friction, reduce pain. Simple.
The problem is that when researchers actually looked at the anatomy, the friction model fell apart. It’s just wrong.
Compression is actually what’s happening
A series of cadaveric studies, most notably by Fairclough and colleagues in 2006 and 2007, demonstrated something that should have changed how we all think about this injury from right then. The IT band doesn’t slide back and forth over the epicondyle. It can’t. It’s not a discrete strap that moves independently. It’s a thickening of the fascia lata, a continuous sheath of connective tissue that wraps the entire thigh. It’s anchored to the femur along much of its length and connected to other tissues that wrap around the quads. There’s no meaningful sliding motion. Let me say that one more time. There’s no meaningful sliding motion. This isn’t friction, ladies and gentlemen.
It’s compression. As the knee moves through about 20 to 30 degrees of flexion (which happens with every single stride when you run and every pedal stroke when you ride), the IT band compresses a layer of richly innervated fat and connective tissue against the lateral epicondyle. This compression that gets applied thousands of times per run irritates the tissue underneath the band. The pain isn’t from friction. It’s from repeated compression of sensitive structures.
This distinction matters because it completely changes how treatment should look. You’re not trying to reduce friction on a surface, you’re trying to reduce compressive load on a specific area of tissue that’s being irritated by repetitive motion.
Foam rolling just doesn’t work
The most important thing about the IT band is that it’s phenomenally stiff. Research on its material properties has shown that you would need forces far beyond what a foam roller or a therapist’s elbow can generate to produce meaningful deformation of the tissue. You can’t bend it. You are not lengthening your IT band. You’re not breaking up adhesions. The tissue is a tendon-like structure that doesn’t yield to manual pressure in any meaningful way. You can’t bend it, stretching it, pull it, twist it, flick it, or bop it.
But foam rolling feels like it helps, right? Why is that? We don’t know for sure, but it’s probably through neurological mechanisms. Temporary pain modulation, changes in perceived tightness, activation of mechanoreceptors, all of these can make you feel better. They’re not nothing. If your IT band feels better for a while, that’s real. But it’s not addressing the underlying problem, so the pain returns. You’re treating the symptom through a transient neurological effect, not changing the structural or biomechanical factors that created the problem. This is like getting your back popped. It feels nice, but it’s not going to actually fix anything about your back.
(I should note that I’m not anti-foam roller in general. There are reasonable uses for it. But stretching the IT band is not one of them, at least not as a primary treatment strategy. If you want the research on what foam rolling actually does and doesn’t do, that’s covered in a separate article in the Recovery & Adaptation section of this library.)
So what actually helps?
If the problem is compressive load on the lateral knee, the question becomes: what controls how much load lands there? The answer is mostly proximal, meaning it’s about what’s happening at your hip. Be like Tulio in The Road to El Dorado. The hip, the hip!
Weakness or poor neuromuscular control in the hip abductors and external rotators (especially gluteus medius) allow the thigh and knee to drift inward during the stance phase of running (when your foot is on the ground). This inward drift (AKA hip adduction and internal rotation) increases tension through the IT band and changes the angle of compression at the knee. If you’ve ever had a gait analysis and been told you have a “crossover” pattern or excessive hip drop, this is what they’re talking about, and it directly loads the lateral knee. This gait pattern smashes the sensitive tissues underneath your IT band, irritating them and leading to pain.
The research consistently points toward hip-focused strengthening and gait modification as the most effective interventions for IT band syndrome, not local treatment to the band itself. A 2020 systematic review by Friede and colleagues confirmed that exercise targeting the hip and knee muscles had the strongest evidence for managing ITBS, and that this approach outperformed passive treatments like stretching, ultrasound, or massage. What’s crazy about that research is that people whose hips got stronger and pain decreased actually had stiffer IT bands after treatment. Their pain went away and their IT bands got stiffer. Excellent evidence for this being about compression, not friction and compliance.
The other major factor is load management. IT band syndrome (like so many other running related injuries) is fundamentally a load problem. Too much compressive stress, too many repetitions, insufficient tissue capacity to handle it. Adjusting training volume, running surfaces, and cadence (higher step rate tends to reduce lateral knee loading) are all part of the picture.
tl;dr
Your IT band isn’t tight. It isn’t sliding. It isn’t something you can stretch or roll into compliance. IT band pain is coming from compression of sensitive tissues at the knee, driven largely by what your hip is doing (or failing to do) during the stance phase. Strengthen the hip. Modify the gait if needed. Manage the load.
The foam roller isn’t your enemy. It just isn’t your solution.
Want the full biomechanical picture? Read the Deep Dive: IT Band Compression, Hip Mechanics, and the Evidence for Load Modification Over Stretching →
Dealing with lateral knee pain that won’t go away? Book a consultation with RVA Endurance PT.

Leave a comment