Deep Dive | Movement & Injury Science
If you haven’t read the Foundation article, IT Band Syndrome Basics, start there. It covers the basics: the friction model is wrong, the compression model is right, the IT band is too stiff to meaningfully deform with a foam roller, and the problem is mostly driven by what happens at the hip. This piece gets into the anatomy, the biomechanics, and the evidence for what actually works.
The anatomy that matters
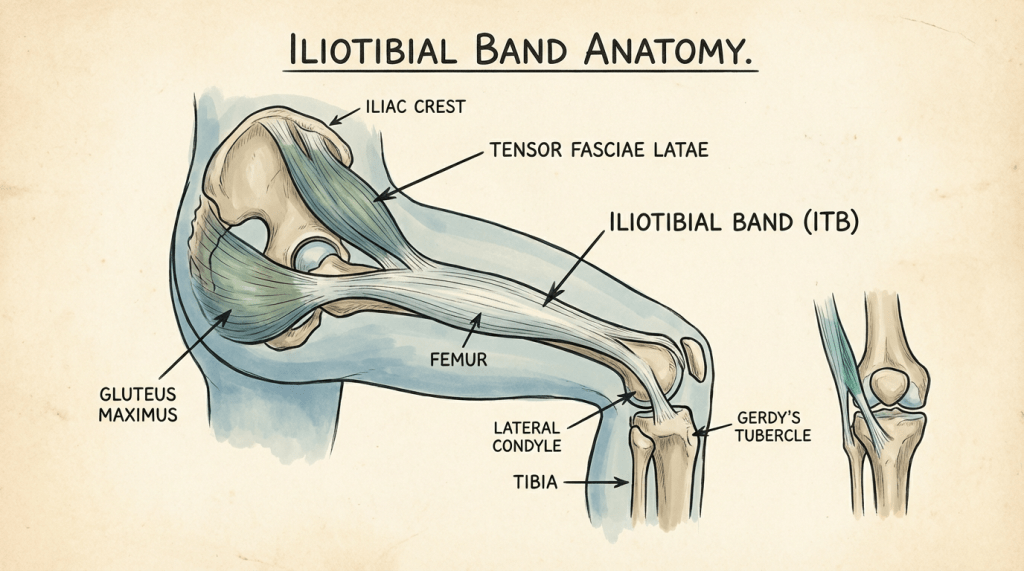
Let’s refresh ourselves with what the IT band actually is. The popular mental model of a thick rubber band running down the side of your leg isn’t accurate and the inaccuracy matters.
The iliotibial (IT) band is not an independent structure. It’s a lateral thickening of the fascia lata, the continuous connective tissue sheath that envelops the entire group of thigh muscles. The IT band originates from the tensor fasciae latae (TFL) and the gluteus maximus, both of which insert into it, and it attaches distally at the lateral tibial tubercle (Gerdy’s tubercle) and through connections to the lateral patellar retinaculum. If you’ve been picturing a strap that’s bolted to the hip at one end and the knee at the other, that’s too simple. It’s more like a structural element in a continuous fascial sleeve, with muscular inputs from above and bony and muscle attachments below and along the way. Think of it as a floor joist, holding the floor up. It’s part of a whole network: subfloor, flooring, rug, etc. It’s a key element, but it’s also just one part that’s attached to all the others.
This matters because the continuity with surrounding fascia means the IT band doesn’t operate in isolation. Forces transmitted through it are influenced by hip abductor and external rotator function, knee flexion angle, and even contralateral pelvic mechanics. It’s part of a system, not an individual cable.
Fairclough and colleagues published two papers (2006 in the Journal of Anatomy, 2007 in the British Journal of Sports Medicine) that fundamentally changed our understanding of IT band pathology. Through detailed cadaveric dissection, they demonstrated that the IT band is firmly anchored to the distal femur via fibrous attachments. It does not slide anteriorly and posteriorly over the lateral epicondyle during knee flexion and extension, which had been the foundational assumption of the friction model for decades. The friction model of IT band pain is wrong.
What Fairclough found instead was a layer of highly vascularized, richly innervated adipose (fat) and loose connective tissue between the the IT band and the lateral epicondyle. During knee flexion (particularly around 20 to 30 degrees, exactly the angle the knee passes through during the stance phase of running), the IT band compresses this tissue against the femur. The nociceptive potential of this tissue, the fact that it has a robust nerve supply, makes it a plausible pain generator. This is the compression model, and it has held up well in subsequent investigations (Geisler, 2020; Friede et al., 2022).
It’s also worth noting that the IT band’s insertion at the knee is not a simple point attachment. It fans out into the lateral retinaculum (a bunch of connective tissue that also attaches to the patella) and has connections to the joint capsule. This means IT band tension influences patellar tracking and overall lateral knee joint mechanics, which is one reason IT band problems can sometimes present with vaguely diffuse lateral knee pain rather than a single pinpoint location. If you’ve ever had a patient or been the patient who says “it hurts on the outside of my knee but I can’t quite put my finger on exactly where,” this anatomy helps explain why.
Why the friction model survived so long
I think this is worth a brief digression, because it illustrates a pattern in science. The friction model was proposed by Renne in 1975 and expanded by various authors over the following decades. It has always been intuitively satisfying. You could feel something that seemed like a snap on the lateral knee during flexion-extension, and the mental image of a band sliding back and forth over a bony prominence was easy to teach and understand. When something “makes sense” like that, it’s really hard to shake it off. Our brains want things to make sense, they’re devoted to that mission. So simple explanations like this are very powerful.
But the key supporting observation, that you could feel or palpate a “snap,” wasn’t actually evidence of sliding. The sensation likely results from the transition of the IT band’s line of pull relative to the epicondyle as the knee flexes, creating an illusion of movement. The band isn’t translating across bone. Its relationship to the epicondyle is changing as the knee angle changes, and the compression zone shifts accordingly. When you bend a joint, tons of things move in concert. The IT band is just one of those things, with sliding over it, under it, and along itself too. It does move some, but not enough to snap around like the model says.
This is one of those cases where a plausible biomechanical narrative got locked in before the anatomical evidence was carefully examined. It happens in exercise science and sports medicine more often than we’d like because it’s just so darn explainable.
The biomechanics of compression
If pain comes from compression of sensitive tissue at the lateral knee, the next question is how can we modify that compression to lessen it? The answer involves three main areas.
Hip mechanics
This is the big one. During the stance phase of running (when your foot is on the ground), the hip abductors (primarily gluteus medius, with contributions from gluteus minimus and TFL) control pelvic drop and femoral adduction (drift toward midline). When these muscles are weak, fatigued, or poorly coordinated, the stance-phase limb tends to drift into greater hip adduction and internal rotation. This is the “knee collapse” or “crossover” pattern you’ll hear coaches and clinicians talk about, though it’s usually subtler during running than during a single-leg squat because of how quickly you’re moving through that zone.
Hip adduction matters for the IT band because it’s pre-tensioned by its proximal attachments to glute max and TFL. As the femur adducts (goes toward midline) beneath a pelvis that’s dropping on the contralateral side, the tension through the IT band increases, and the compression against the lateral epicondyle intensifies. IT band is pulled, tissue is squished. Noehren and colleagues (2007) demonstrated that runners who developed IT band syndrome exhibited significantly greater hip adduction during stance phase compared to controls who didn’t get it. This was a prospective study, meaning the biomechanical pattern was identified before the injury developed, so it’s stronger evidence than the more common retrospective design.
If you’ve spent any time on running forums or listening to coaching podcasts (TrainerRoad, Strength Running, Running Rogue, etc.), you’ve heard the advice to “strengthen your glutes.” That advice is correct, but the reasoning people give for it is often vague or wrong. It’s not that your glutes are “inactive” or “not firing” (this is a myth. Your glutes are firing during running or you would fall over). It’s that their capacity may be insufficient relative to the demands of your training volume, or their timing and coordination during the gait cycle may be less than optimal. The distinction between “weak” and “poorly coordinated” matters for how you rehab the problem.
Step width and crossover gait
A narrow step width during running, sometimes called a “crossover” gait, increases hip adduction and lateral knee loading. Runners with ITBS have been shown to run with a narrower step width compared to uninjured runners (Meardon & Derrick, 2014). Widening your step width, which can be cued during gait retraining, reduces the impingement zone and decreases IT band strain.
This is one of the simpler gait modifications to implement and has good evidence behind it. If you run on a road and notice your feet are landing close to a center line (or even crossing it), you may be a candidate for this adjustment. That said, I want to pause to say that gait retraining should be done deliberately and ideally with someone watching you. Making changes to running form without guidance is really difficult and can sometimes just trade one problem for another.
Cadence
Higher running cadence (more steps per minute at the same speed) tends to reduce ground contact time, decrease load at the knee, and reduce hip adduction. A 2011 study by Heiderscheit and colleagues found that a 5 to 10% increase in step rate reduced energy absorption at the hip and knee and decreased peak hip adduction angle. This has become one of the most commonly mentioned gait modification strategies in running medicine research, and it’s well-supported.
You’ll hear the “180 steps per minute” number thrown around a lot in popular running content. That target is overly simplistic and not evidence-based as a universal prescription (it traces back to an observation by Jack Daniels of elite runners at the 1984 Olympics). What the research actually supports is a relative increase from your self-selected cadence, typically 5 to 10%. If you naturally run at 160 steps per minute, you don’t need to get to 180. You need to get to 168 to 176. The individual starting point matters.
Bike fit (for cyclists)
IT band issues in cyclists deserve a brief mention because the mechanism is somewhat different. On a bike, the repetitive knee flexion-extension pattern through the compression zone is present (especially at lower cadences with higher forces), but hip mechanics operate differently in a constrained position.
Saddle height, cleat position, and Q-factor (the lateral distance between the pedals) all influence lateral knee loading. A saddle that’s too high increases knee extension at the bottom of the pedal stroke, increasing IT band tension. Cleats with insufficient float or improper rotational alignment can lock the foot into a position that drives tibial rotation and alters knee tracking. If you’re a cyclist with lateral knee pain, a proper bike fit is not optional. It’s the equivalent of the gait analysis for a runner.
I’ve been thinking a lot about bike fitting lately, and the thing that stands out is how many cyclists are riding positions that were set by shop employees during purchase and never revisited. A 2mm cleat adjustment can change the entire loading profile at the knee over the course of thousands of pedal strokes. It’s worth getting it done by a pro.
What the evidence says about treatment
What works
Hip-focused strengthening. This is the intervention with the most consistent evidence. A 2022 systematic review by Friede and colleagues found that exercise programs targeting hip abduction, external rotation, and knee extensor strength were the most effective conservative treatment for ITBS. Other work by Willy and Davis (2011) demonstrated that hip-focused rehab improved both symptoms and the underlying biomechanical patterns (reduced hip adduction during running) and that these changes were maintained at a 6-month follow-up visit.
The exercises themselves are boring. Clamshells, side-lying hip abduction, single-leg bridges, single-leg squats, lateral band walks. The key is progressive loading. Start with low-load, isolation work and progress to dynamic, weight-bearing, sport-specific tasks. If you’re doing clamshells for six months and never progressing beyond them, you’re not building the capacity your hip needs during running. Your hip has to be strong in the context of stance-phase demands, which means that, eventually, your rehab has to include single-leg loading at speed. The Myrtl routine is great, but it’s not an endpoint. You have to advance exercises to continue to improve
Gait retraining. Step width modification and cadence changes both have good evidence, as discussed above. These can be implemented during the rehab process and may have lasting effects on running mechanics.
Load management. This is perhaps the most important intervention and the one athletes resist the most. IT band syndrome is a load-related injury. The tissue is being compressed beyond its capacity to tolerate it. Reducing running volume, adjusting intensity distribution, changing surfaces or pitches (downhill running increases lateral knee loading significantly), and introducing more rest days are all part of managing the load side of the equation. If you only strengthen the hip and don’t address the training load that created the problem, you’re playing basketball defense with one hand.
For athletes who follow structured training plans, the load management conversation needs to be integrated with the training plan. It’s not just “run less.” It’s “how do we modify volume and intensity distribution to allow tissue recovery while preserving the aerobic base you’ve built?”
What doesn’t work (or works less than people think)
Foam rolling the IT band. We covered this in the Foundation article, but to add the evidence detail. Chaudhry and colleagues (2008) modeled the forces required to produce even 1% compression and shear of the IT band and found that they far exceed what manual techniques can deliver. The band is simply too stiff. The perceived benefit is likely a transient neurological effect (pain gate modulation, changes in perceived stiffness), but not a structural change.
Stretching the IT band. Same problem as above. The material properties of the IT band make it resistant to elongation. That’s really the point of the band, is to pre-tension the limb and not stretch. Falvey and colleagues (2010) demonstrated that even aggressive stretching protocols produced negligible changes in IT band length. You’re more likely stretching adjacent structures (hip flexors, TFL, glute max) when you perform “IT band stretches,” which isn’t bad, but it’s not doing what you think it’s doing.
Corticosteroid injection. There is some evidence of short-term pain relief, but no evidence of long-term benefit and concerns about tissue quality degradation with repeated injections. A 2022 study by Mautner and colleagues found that ultrasound-guided corticosteroid injection provided significant pain relief at 4 weeks but no difference from placebo at 12 weeks. It might have a role in managing acute flares to facilitate rehab participation, but it’s not a standalone treatment.
Ultrasound, iontophoresis, and other passive modalities. Insufficient evidence to recommend any of them. The Friede et al. (2022) systematic review found no support for these interventions as primary treatments for ITBS.
Return to run
One of the most common questions I get from runners with ITBS is some version of “when can I start running again?” The honest answer is that there isn’t a universal return-to-run protocol specific to ITBS. We don’t have a one size fits all plan. What we do have are general principles from the broader return-to-sport research and some emerging ITBS-specific guidance.
The general framework I use is this. Do pain-free daily activities first, then progressively load through walking and eventually run-walk intervals, with volume increases governed by symptom response rather than arbitrary timelines. As in, no guarantee that you’ll run three miles next week, but if you feel good, go ahead. The hip strengthening work should be well-established before returning to running, not something you start at the same time. And the gait modifications (if indicated) should be practiced at low-intensity running speeds before you try to maintain them during a tempo session.
I’ll note that many runners with ITBS don’t need to stop running. If the pain is intensity-dependent or volume-dependent, modifying the training load (shorter runs, avoiding downhill, slower pace) can sometimes keep you running while the rehab progresses. This requires a case-by-case assessment, which is part of why working with someone who understands both the biomechanics and your training goals is valuable.
What we still don’t know
We don’t have a strong understanding of why some runners develop ITBS and others with similar biomechanical profiles don’t. The prospective studies (like Noehren et al., 2007) identified associations, not clean causal chains. There’s likely a threshold effect where tissue capacity and training load interact, but we don’t have good tools for quantifying that threshold in individual athletes.
The role of the TFL versus glute max in tensioning the IT band during running is still being clarified. Some recent work suggests that TFL overactivity relative to glute max may be a contributing factor, but the clinical implications of this are not yet settled.
The long-term outcomes of gait retraining for ITBS are not well studied. We have good short-term data showing that biomechanical changes are achievable and associated with symptom improvement, but whether these changes persist over years of training and whether they truly prevent recurrence is an open question.
The conclusion
IT band syndrome is a compression injury, not a friction injury. The tissue under the IT band is being repeatedly loaded beyond its capacity, driven primarily by hip mechanics and influenced by step width, cadence, training volume, and (for cyclists) bike fit. The evidence supports hip-focused strengthening, gait modification, and load management as the core treatment strategy. Foam rolling and stretching the IT band are not effective treatments, though they’re not harmful if you enjoy them and they make you feel better.
The most common mistake I see is athletes treating this as a local problem at their knee when it’s really a system problem driven from above and amplified by training load. Fix the hip. Modify the gait if needed. Respect the load. The knee is just where the pain lives, it’s rarely where the problem starts.
References
Baker, R. L., & Fredericson, M. (2016). Iliotibial band syndrome in runners: biomechanical implications and exercise interventions. Physical Medicine and Rehabilitation Clinics of North America, 27(1), 53-77.
Chaudhry, H., Schleip, R., Ji, Z., Bukiet, B., Maney, M., & Findley, T. (2008). Three-dimensional mathematical model for deformation of human fasciae in manual therapy. Journal of the American Osteopathic Association, 108(8), 379-390.
Fairclough, J., Hayashi, K., Toumi, H., et al. (2006). The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. Journal of Anatomy, 208(3), 309-316.
Fairclough, J., Hayashi, K., Toumi, H., et al. (2007). Is iliotibial band syndrome really a friction syndrome? Journal of Science and Medicine in Sport, 10(2), 74-76.
Falvey, E. C., Clark, R. A., Franklyn-Miller, A., Bryant, A. L., Briggs, C., & McCrory, P. R. (2010). Iliotibial band syndrome: an examination of the evidence behind a number of treatment options. Scandinavian Journal of Medicine and Science in Sports, 20(4), 580-587.
Ferber, R., Noehren, B., Hamill, J., & Davis, I. S. (2010). Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. Journal of Orthopaedic and Sports Physical Therapy, 40(2), 52-58.
Friede, M. C., Klauser, A., Groscurth, R., & Fink, C. (2022). Conservative treatment of iliotibial band syndrome in runners: are we heading in the right direction? A systematic review. Current Reviews in Musculoskeletal Medicine, 15(4), 215-229.
Geisler, P. R. (2020). Iliotibial band impingement syndrome: a narrative review. Current Sports Medicine Reports, 19(9), 348-352.
Heiderscheit, B. C., Chumanov, E. S., Michalski, M. P., Wille, C. M., & Ryan, M. B. (2011). Effects of step rate manipulation on joint mechanics during running. Medicine and Science in Sports and Exercise, 43(2), 296-302.
Meardon, S. A., & Derrick, T. R. (2014). Effect of step width manipulation on tibial stress during running. Journal of Biomechanics, 47(11), 2738-2744.
Noehren, B., Davis, I., & Hamill, J. (2007). ASB Clinical Biomechanics Award Winner 2006: Prospective study of the biomechanical factors associated with iliotibial band syndrome. Clinical Biomechanics, 22(9), 951-956.
Willy, R. W., & Davis, I. S. (2011). The effect of a hip-strengthening program on mechanics during running and during a single-leg squat. Journal of Orthopaedic and Sports Physical Therapy, 41(9), 625-632.
New to this topic? Start with the Foundation: IT Band Syndrome Basics →
Lateral knee pain that keeps coming back? I work with runners and cyclists in Richmond, VA and remotely. Book a consultation with RVA Endurance PT.

Leave a comment